- Get started
- Learn the Program

What’s the evidence for vitamin D and natural sunlight with MS?
Find out about the evidence about vitamin D, sunlight and MS.
Explore this sectionThe recognised importance of natural sunlight in aiding sleep, stress and our natural circadian rhythms for optimal health, and of having healthy levels of vitamin D throughout the year, has been increasing in recent years. Global public health messaging highlights the importance of sunlight and vitamin D in supporting health (Wacker & Holick 2013).
‘A three-part strategy of increasing food fortification programs with vitamin D, sensible sun exposure recommendations and encouraging ingestion of a vitamin D supplement when needed should be implemented to prevent global vitamin D deficiency and its negative health consequences’ (Wacker & Holick 2013).
Vitamin D deficiency is a global concern (Roth 2018). Deficiency is classed by the British Medical Journal as less that 20nmol/L whilst insufficiency is between 52-72 nmol/L (BMJ 2025). Analysis of 7.9 million participants across the globe found that 47.9% had levels below 50 nmol/L and 76.6% lower than 75 nmol/L (Cui 2023). Levels below 50 mnol/L are common across Europe (20-60%) and the Middle East (up to 80%) (Lips 2019).
Whilst there are conflicting findings across the breadth of studies into MS and vitamin D, there is sufficient evidence to highlight a definitive interrelationship between vitamin D levels and both the onset and progression of MS (Gandhi 2021) and the role of vitamin D in promoting brain health is also important. A recent review found vitamin D has a neuroprotective role in brain health, specifically in supporting remyelination and/ or preventing demyelination; particularly important for those with MS (Sangha 2023).

High levels of vitamin D and disease activity
Research into vitamin D has been conflicting; some studies find that higher vitamin D levels are associated with lower relapse rates compared with lower levels (Pierrot-Deseilligny 2012; Scott 2013; Runia 2012; Simpson 2010), but some found no correlation (Hanaei 2021; Cassard 2023).
High vitamin D levels at MS diagnosis have been associated with slower disease progression and less disease activity compared to a poorer prognosis in those with low levels at diagnosis (Asherio 2014). Across people with clinically-isolated syndrome (CIS) and relapsing-remitting MS (RRMS), higher levels of vitamin D have been found to coexist with lower risk of developing new lesions in the brain, including gadolinium-enhancing lesions (Mowry 2012).
Low levels of vitamin D levels in MS
In reviewing the role of low levels of vitamin D levels in MS, there is more consistency. A comprehensive review found that low levels of vitamin D correlate with poorer outcomes and more disease activity in people living with MS (Sintzel, Rametta & Reder 2018).
This included:
- increased risk of relapse (Runia 2012) and lower odds of remaining relapse free (Smolders 2008),
- increased disease activity (Wang 2018)
- greater disability and disease severity (Mowry 2012; Smolders 2008, Harandi 2012, Shahbeigi 2013)
- conversion from CIS to clinically definite MS (CDMS) (Martinelli 2013),
- and poorer nonverbal long-term memory performance (Koven 2013)
In people with relapsing-remitting MS, pre-disease-modifying treatment, lower vitamin D was associated with less likelihood of NEDA (no evidence of disease activity) after two years. Furthermore, levels under 20 ng/mL (or 50nmol/L) related to a two-fold increased risk of disease activity (Giordano 2024).
Two studies seeking to establish whether vitamin D supplementation in clinically isolated syndrome (CIS) could slow or prevent progression to MS had conflicting findings: one found that intermittent high doses (100,000 units) of vitamin D slowed disease progression and delayed development of new lesions (Thouvenot 2024), the other found that daily supplementation of up to 10,000 units (other cohorts took 1,000 and 5,000 respectively) did not (Butzkueven 2024). Key differences in the studies included length of time, amount and frequency of supplementation and baseline vitamin D levels, suggesting that the role of supplementation may be more nuanced.
There are clearly interactions between vitamin D and MS activity that still need to be better understood, and whilst we cannot draw firm conclusions around specifics, we can see that vitamin D levels have an important role to play in MS disease activity, perhaps particularly in its earliest stages.

Vitamin D and risk of MS
Overcoming MS advocate for a healthy lifestyle across the whole family, both as a means of supporting the person living with MS in their ‘brain-healthy lifestyle’ (Giovannoni 2023) and to protect each member of the family from ill-health themselves.
‘The findings from our review indicate a strong correlation between the insufficiency of vitamin D and the onset and progression of MS.’ (Gandhi 2021)
A systematic review and meta-analysis summarised that individuals with vitamin D deficiency (less than 50nmol/L) had more than double the risk of MS than those with ‘sufficient’ vitamin D levels (Balasooriya 2024).
Reviewing sun exposure in childhood and risk of MS, a large study found that decreased sunlight exposure in childhood was associated with almost 50% increased risk of MS, whilst children who had both low sun exposure year round, and high sun protection use had a 76% increased risk compared with those who had high sun exposure and low sun protection (Magalhaes 2018).
Guidance on supplementation
A meta-analysis of 12 studies across 940 people concluded ‘it may have a therapeutic role in the treatment of MS’ (McLaughlin 2018) and maintaining a ‘healthy level’ in people with MS often requires the use of supplementation (NICE 2016; Neale 2024). A recent review highlights the importance of preventing vitamin D deficiency in those with MS (Plantone 2022). Suggested healthy levels are of around or above 100 nmol/L (Smolders 2019) with 100-150 nmol/L being closer to the optimal levels found in healthy hunter-gatherer tribes around the planet often noted for their health and longevity (Gandhi 2021).
There is no single agreed dose for supplementation; 4,000 units per day is often recommended by neurologists in the UK (Dobson 2018) and is also echoed in guidance on bone health (Royal Osteoporosis Society 2020 whilst between 6,000-10,000 units may be needed to maintain blood serum levels of 100-150 mnol/L (Gandhi 2021).
A consensus paper across UK neurologists notes that safe and effective supplementary dosage should be ideally discussed with a clinician and that supplement level taken for several weeks before a blood serum level test, after which the clinician will advise on supplementation going forward. Achieving optimal, safe levels of vitamin D will vary across individuals, and those with epilepsy or who are pregnant may need higher levels of supplementation (Dobson 2018).
‘The conclusion is that increasing our vitamin D intake to maintain blood 25(OH)D levels of at least 30 ng/mL (75 nmol/L), and preferably 40-60 ng/mL (100-150 nmol/L) for optimal overall health benefits, is not associated with any negative consequences.’ (Gandhi 2021)
In terms of safety, a daily dose of up to 10,400 units is considered safe and well tolerated (Sotirchos 2016; Butzkueven 2024) whilst a recent study supplementing with far higher amounts of 100,000 units every fortnight was also found to be safe and well tolerated (Thouvenot 2024). (There have been relatively few cases of hypercalcaemia caused by high levels of vitamin D and where they occur they are very high levels for a sustained period, for example the deVincentis case study found average dosing of 130,000 units daily for 20 months resulting in serum blood levels of 940 mnol/L (deVincentis 2020; Bell 2013).
Despite this guidance, a Cochrane review of 12 randomised control trials (RCTs) concluded that there was no high-quality evidence for the use of vitamin D supplementation to support patient outcomes including relapse, disability or lesions, although it did confirm safety of dosing across all studies reviewed (Jagannath 2018). Another recent literature review concluded similarly (Boltjes 2021). This both highlights the challenges of capturing nuances in randomised-control trials, and the need for still more research to support our understanding of the relationship between vitamin D and MS, and what that means for healthy decisions around activities and supplementation.

Sunlight to support health – beyond vitamin D
Safe sunlight exposure is one way to increase vitamin D levels, although in many parts of the world, it is difficult to get sufficient vitamin D from sunlight exposure alone; for example, between October and March in the UK (NICE 2016). Advice from UK to Australia highlights the need to discuss vitamin D supplementation rather than choosing to use sunlight as the only form of vitamin D access (NICE 2016; Neale 2024).
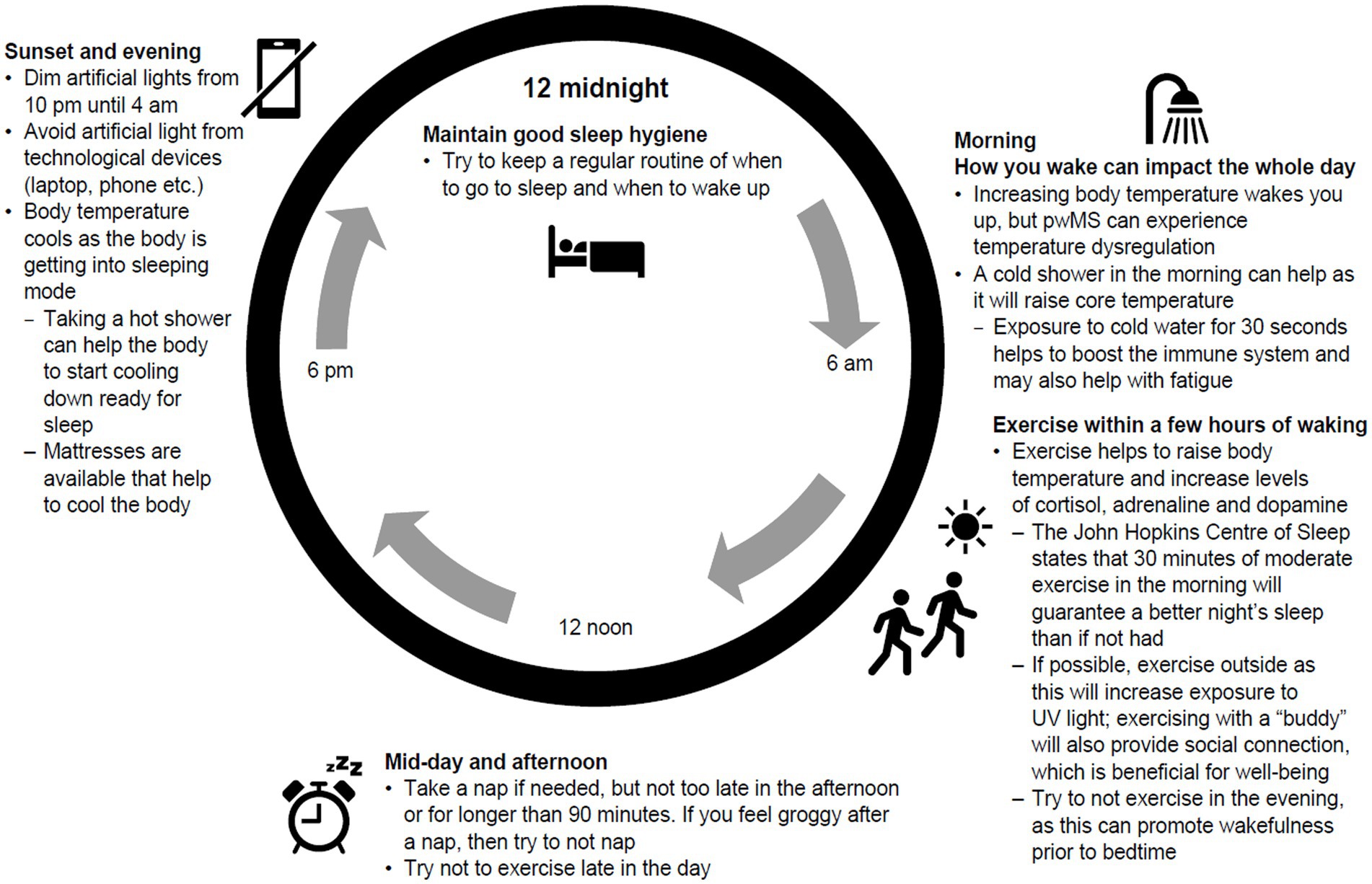
However, sunlight has a broader role to play in symptom management for MS from circadian health to photoneuroimmunologic interplay (Hart 2009). Sunlight exposure in the early morning and late evening can support healthy circadian function (Reddy 2023), optimising melatonin production and supporting good quality sleep (Giovannoni 2023 – figure 2), which in turn can aid symptoms like mood, pain, fatigue and cognition (Giovannoni 2023). The potential benefits of a healthy circadian clock for people with MS have even prompted a recent paper to consider chronotherapeutic approaches to supporting the immune, endocrine and digestive systems (Pivovarova 2023).
We review our content regularly. Last review 12 February 2025. Next review by 12 August 2026.
References
Ascherio, A., Munger, K. L., White, R., Köchert, K., Simon, K. C., Polman, C. H., Freedman, M. S., Hartung, H. P., Miller, D. H., Montalbán, X., Edan, G., Barkhof, F., Pleimes, D., Radü, E. W., Sandbrink, R., Kappos, L., & Pohl, C. (2014). Vitamin D as an early predictor of multiple sclerosis activity and progression. JAMA neurology, 71(3), 306–314. https://doi.org/10.1001/jamaneurol.2013.5993
Balasooriya, Namal N. et al. The association between vitamin D deficiency and multiple sclerosis: an updated systematic review and meta-analysis, Multiple Sclerosis and Related Disorders, Volume 90, 105804 October 2024, DOI: 10.1016/j.msard.2024.105804
Bell, D. A., Crooke, M. J., Hay, N., & Glendenning, P. (2013). Prolonged vitamin D intoxication: presentation, pathogenesis and progress. Internal medicine journal, 43(10), 1148–1150. https://doi.org/10.1111/imj.12269
Boltjes, R., Knippenberg, S., Gerlach, O., Hupperts, R., & Damoiseaux, J. (2021). Vitamin D supplementation in multiple sclerosis: an expert opinion based on the review of current evidence. Expert Review of Neurotherapeutics, 21(6), 715–725. https://doi.org/10.1080/14737175.2021.1935878
British Medical Journal, BMJ Best Practice, last updated 4 June 2024, last reviewed 15 January 2025, accessed Vitamin D deficiency – Symptoms, diagnosis and treatment | BMJ Best Practice
Butzkueven, H., Ponsonby, A.-L., Stein, M. S., Lucas, R. M., Mason, D., Broadley, S., Kilpatrick, T., Lechner-Scott, J., Barnett, M., Carroll, W., Taylor, B. V., & the PREVANZ Investigators. (2024). Vitamin D did not reduce multiple sclerosis disease activity after a clinically isolated syndrome. Brain, 147, 1206–1215. https://doi.org/10.1093/brain/awad409
Cassard SD, Fitzgerald KC, Qian P, Emrich SA, Azevedo CJ, Goodman AD, Sugar EA, Pelletier D, Waubant E, Mowry EM. High-dose vitamin D3 supplementation in relapsing-remitting multiple sclerosis: a randomised clinical trial. EClinicalMedicine. 2023 Apr 13;59:101957. doi: 10.1016/j.eclinm.2023.101957. PMID: 37125397; PMCID: PMC10130605.
Cui A, Zhang T, Xiao P, Fan Z, Wang H, Zhuang Y. Global and regional prevalence of vitamin D deficiency in population-based studies from 2000 to 2022: A pooled analysis of 7.9 million participants. Front Nutr. 2023 Mar 17;10:1070808. doi: 10.3389/fnut.2023.1070808. PMID: 37006940; PMCID: PMC10064807.
De Vincentis, S., Russo, A., Milazzo, M., Lonardo, A., De Santis, M. C., Rochira, V., Simoni, M., & Madeo, B. (2021). How Much Vitamin D is Too Much? A Case Report and Review of the Literature. Endocrine, metabolic & immune disorders drug targets, 21(9), 1653–1659. https://doi.org/10.2174/1871530320666201007152230
Dobson R, Cock HR, Brex P, et al Vitamin D supplementation Practical Neurology 2018;18:35-42.
Gandhi F, Jhaveri S, Avanthika C, Singh A, Jain N, Gulraiz A, Shah P, Nasir F. Impact of Vitamin D Supplementation on Multiple Sclerosis. Cureus. 2021 Oct 5;13(10):e18487. doi: 10.7759/cureus.18487. PMID: 34754649; PMCID: PMC8567111.
Giordano A, Clarelli F, Pignolet B, Mascia E, Sorosina M, Misra K, Ferrè L, Bucciarelli F, Manouchehrinia A, Moiola L, Martinelli V, Rocca MA, Liblau R, Filippi M, Esposito F. Vitamin D affects the risk of disease activity in multiple sclerosis. J Neurol Neurosurg Psychiatry. 2024 Jul 14:jnnp-2024-334062. doi: 10.1136/jnnp-2024-334062. Epub ahead of print. PMID: 39004505.
Giovannoni G, Ford HL, Schmierer K, Middleton R, Stennett AM, Pomeroy I, Fisniku L, Scalfari A, Bannon C, Stross R, Hughes S, Williams A, Josephs S, Peel C, Straukiene A. MS care: integrating advanced therapies and holistic management. Front Neurol. 2024 Jan 30;14:1286122. doi: 10.3389/fneur.2023.1286122. PMID: 38351950; PMCID: PMC10862341.
Hanaei S, Sahraian MA, Mohammadifar M, Ramagopalan SV, Ghajarzadeh M. Effect of Vitamin D Supplements on Relapse Rate and Expanded Disability Status Scale (EDSS) in Multiple Sclerosis (MS): A Systematic Review and Meta-Analysis. Int J Prev Med. 2021 May 15;12:42. doi: 10.4103/ijpvm.IJPVM_208_20. PMID: 34211673; PMCID: PMC8223916.
Hart, P.H., Finlay-Jones, J.J., Gorman, S. (2009). Photoneuroimmunology: Modulation of the Neuroimmune System by UV Radiation. In: Granstein, R.D., Luger, T.A. (eds) Neuroimmunology of the Skin. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-540-35989-0_12
Jagannath VA, Filippini G, Di Pietrantonj C, Asokan GV, Robak EW, Whamond L, Robinson SA. Vitamin D for the management of multiple sclerosis. Cochrane Database Syst Rev. 2018 Sep 24;9(9):CD008422. doi: 10.1002/14651858.CD008422.pub3. PMID: 30246874; PMCID: PMC6513642.
Koven, N. S., Cadden, M. H., Murali, S., & Ross, M. K. (2013). Vitamin D and long-term memory in multiple sclerosis. Cognitive and behavioral neurology : official journal of the Society for Behavioral and Cognitive Neurology, 26(3), 155–160. https://doi.org/10.1097/WNN.0000000000000009
Lips P, Cashman KD, Lamberg-Allardt C, Bischoff-Ferrari HA, Obermayer-Pietsch B, Bianchi ML, Stepan J, El-Hajj Fuleihan G, Bouillon R. Current vitamin D status in European and Middle East countries and strategies to prevent vitamin D deficiency: a position statement of the European Calcified Tissue Society. Eur J Endocrinol. 2019 Apr;180(4):P23-P54. doi: 10.1530/EJE-18-0736. PMID: 30721133.
Magalhaes S, Pugliatti M, Riise T, Myhr KM, Ciampi A, Bjornevik K, Wolfson C. Shedding light on the link between early life sun exposure and risk of multiple sclerosis: results from the EnvIMS Study. Int J Epidemiol. 2019 Aug 1;48(4):1073-1082. doi: 10.1093/ije/dyy269. PMID: 30561654; PMCID: PMC6693814.
Martinelli, V., Dalla Costa, G., Colombo, B., Dalla Libera, D., Rubinacci, A., Filippi, M., Furlan, R., & Comi, G. (2014). Vitamin D levels and risk of multiple sclerosis in patients with clinically isolated syndromes. Multiple sclerosis (Houndmills, Basingstoke, England), 20(2), 147–155. https://doi.org/10.1177/1352458513494959
McLaughlin L, Clarke L, Khalilidehkordi E, Butzkueven H, Taylor B, Broadley SA. Vitamin D for the treatment of multiple sclerosis: a meta-analysis. J Neurol. 2018 Dec;265(12):2893-2905. doi: 10.1007/s00415-018-9074-6. Epub 2018 Oct 3. PMID: 30284038.
Mowry EM, Waubant E, McCulloch CE, Okuda DT, Evangelista AA, Lincoln RR, Gourraud PA, Brenneman D, Owen MC, Qualley P, Bucci M, Hauser SL, Pelletier D. Vitamin D status predicts new brain magnetic resonance imaging activity in multiple sclerosis. Ann Neurol. 2012 Aug;72(2):234-40. doi: 10.1002/ana.23591. PMID: 22926855; PMCID: PMC3430977.
National Insititute of Health and Care Excellence (NICE), Sunlight exposure: risks and benefits, 9 Feb 2016, updated 2024, https://www.nice.org.uk/guidance/ng34
Neale RE, Beedle V, Ebeling PR, Elliott T, Francis D, Girgis CM, Gordon L, Janda M, Jones G, Lucas RM, Mason RS, Monnington PK, Morahan J, Paxton G, Sinclair C, Shumack S, Smith J, Webb AR, Whiteman DC. Balancing the risks and benefits of sun exposure: A revised position statement for Australian adults. Aust N Z J Public Health. 2024 Feb;48(1):100117. doi: 10.1016/j.anzjph.2023.100117. Epub 2024 Feb 12. PMID: 38350754.
Pierrot-Deseilligny C, Rivaud-Péchoux S, Clerson P, de Paz R, Souberbielle JC. Relationship between 25-OH-D serum level and relapse rate in multiple sclerosis patients before and after vitamin D supplementation. Ther Adv Neurol Disord. 2012 Jul;5(4):187-98. doi: 10.1177/1756285612447090. PMID: 22783368; PMCID: PMC3388527.
Pivovarova-Ramich, O., Zimmermann, H. G., & Paul, F. (2023). Multiple sclerosis and circadian rhythms: Can diet act as a treatment?. Acta physiologica (Oxford, England), 237(4), e13939. https://doi.org/10.1111/apha.13939
Plantone D, Primiano G, Manco C, Locci S, Servidei S, De Stefano N. Vitamin D in Neurological Diseases. Int J Mol Sci. 2022 Dec 21;24(1):87. doi: 10.3390/ijms24010087. PMID: 36613531; PMCID: PMC9820561
Reddy, S., Reddy, V., & Sharma, S. (2023). Physiology, Circadian Rhythm. In StatPearls. StatPearls Publishing.
Roth DE, Abrams SA, Aloia J, Bergeron G, Bourassa MW, Brown KH, Calvo MS, Cashman KD, Combs G, De-Regil LM, Jefferds ME, Jones KS, Kapner H, Martineau AR, Neufeld LM, Schleicher RL, Thacher TD, Whiting SJ. Global prevalence and disease burden of vitamin D deficiency: a roadmap for action in low- and middle-income countries. Ann N Y Acad Sci. 2018 Oct;1430(1):44-79. doi: 10.1111/nyas.13968. Epub 2018 Sep 18. PMID: 30225965; PMCID: PMC7309365.
Royal Osteoporosis Society, Vitamin D and Bone Health: a practical clinical guideline for patient management, 2020 accessed via ros-vitamin-d-and-bone-health-in-adults-february-2020.pdf
Runia TF, Hop WC, de Rijke YB, Buljevac D, Hintzen RQ. Lower serum vitamin D levels are associated with a higher relapse risk in multiple sclerosis. Neurology. 2012 Jul 17;79(3):261-6. doi: 10.1212/WNL.0b013e31825fdec7. Epub 2012 Jun 13. PMID: 22700811.
Sangha A, Quon M, Pfeffer G, Orton SM. The Role of Vitamin D in Neuroprotection in Multiple Sclerosis: An Update. Nutrients. 2023 Jun 30;15(13):2978. doi: 10.3390/nu15132978. PMID: 37447304; PMCID: PMC10346708.
Scott TF, Hackett CT, Dworek DC, Schramke CJ. Low vitamin D level is associated with higher relapse rate in natalizumab treated MS patients. J Neurol Sci. 2013 Jul 15;330(1-2):27-31. doi: 10.1016/j.jns.2013.03.020. Epub 2013 Apr 18. PMID: 23602794.
Simpson S Jr, Taylor B, Blizzard L, Ponsonby AL, Pittas F, Tremlett H, Dwyer T, Gies P, van der Mei I. Higher 25-hydroxyvitamin D is associated with lower relapse risk in multiple sclerosis. Ann Neurol. 2010 Aug;68(2):193-203. doi: 10.1002/ana.22043. PMID: 20695012
Sintzel MB, Rametta M, Reder AT. Vitamin D and Multiple Sclerosis: A Comprehensive Review. Neurol Ther. 2018 Jun;7(1):59-85. doi: 10.1007/s40120-017-0086-4. Epub 2017 Dec 14. PMID: 29243029; PMCID: PMC5990512.
Smolders J, Torkildsen Ø, Camu W, Holmøy T. An Update on Vitamin D and Disease Activity in Multiple Sclerosis. CNS Drugs. 2019 Dec;33(12):1187-1199. doi: 10.1007/s40263-019-00674-8. PMID: 31686407; PMCID: PMC6890630.
Sotirchos ES, Bhargava P, Eckstein C, Van Haren K, Baynes M, Ntranos A, Gocke A, Steinman L, Mowry EM, Calabresi PA. Safety and immunologic effects of high- vs low-dose cholecalciferol in multiple sclerosis. Neurology. 2016 Jan 26;86(4):382-90. doi: 10.1212/WNL.0000000000002316. Epub 2015 Dec 30. PMID: 26718578; PMCID: PMC4776090.
Sîrbe C, Rednic S, Grama A, Pop TL. An Update on the Effects of Vitamin D on the Immune System and Autoimmune Diseases. Int J Mol Sci. 2022 Aug 29;23(17):9784. doi: 10.3390/ijms23179784. PMID: 36077185; PMCID: PMC9456003.
Thouvenot E, et al, “High-dose cholecalciferol reduces multiple sclerosis disease activity after a clinically isolated syndrome: results of a 24-month placebo-controlled randomized trial (D-Lay-MS).” Oral presentation, European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS) annual meeting, Sept. 18-20 2024 (pre-publication) review presentation accessed https://distribute.congrex.com/from.storage?image=YfwaZin-RHjQeKJF3w_2g4u0KdCVsJktWSb0msXKvyF1IvLSyx6NvKj-bzciXM8w0
Wacker M, Holick MF. Sunlight and Vitamin D: A global perspective for health. Dermatoendocrinol. 2013 Jan 1;5(1):51-108. doi: 10.4161/derm.24494. PMID: 24494042; PMCID: PMC3897598.
Wang C, Zeng Z, Wang B, Guo S. Lower 25-Hydroxyvitamin D Is Associated with Higher Relapse Risk in Patients with Relapsing-Remitting Multiple Sclerosis. J Nutr Health Aging. 2018;22(1):38-43. doi: 10.1007/s12603-017-0894-3. PMID: 29300420.
Further reading
- Learn the Program













{kind=link}