
Paper looks at diet quality and the risk of further relapse after someone’s first demyelinating event, comparing three dietary patterns.
As many of us know only too well, the subject of diet and MS can be a frustrating one. First of all, there are numerous regimens to choose from, permitting or excluding different food groups, some with opposing views on the basic science behind the condition itself, and often underpinned by limited scientific evidence to support their claims.
And there it is, that word, “evidence”. The ever-present thorn in the side of those of us who firmly believe in the power of the Overcoming MS program, and its ability to allow us to live well with MS. How often do we hear that over-used catchphrase “there’s no evidence for any of that”, thrown casually at us by our MS team? The very real power of the “nocebo” effect, to steal hope from us, and to set us back on our quest to be well.
Often that expression is used simply through a lack of awareness of the evidence base, or perhaps from a fundamental lack of understanding of the core principles of evidence-based medicine (EBM) and how it actually functions. One cannot easily use “fake steak” in a randomised controlled trial, for example, or “mimic mindfulness”. I am being a little facetious, but I hope you get my point. It has not been the case of there being “no evidence” for over 30 years, when Professor Swank’s original paper was published in “The Lancet” in 1990, and arguably much longer if you look at the foundations behind Swank’s pioneering trial. It is the case however, that the results, quality and concordance of many studies into diet and lifestyle in MS have been questioned. Sadly, all too often, it is the people with MS themselves that suffer as a result.
But this demonstrates the difficulty in undertaking lifestyle-related research. These studies are significantly harder to conduct and measure; for a start, they often rely on the subjects not simply taking a pill each day, but rather to often recall and honestly record the data themselves. It is also more difficult to adhere to a “diet” than to take a tablet over a long-term period, and it is easier to cheat.
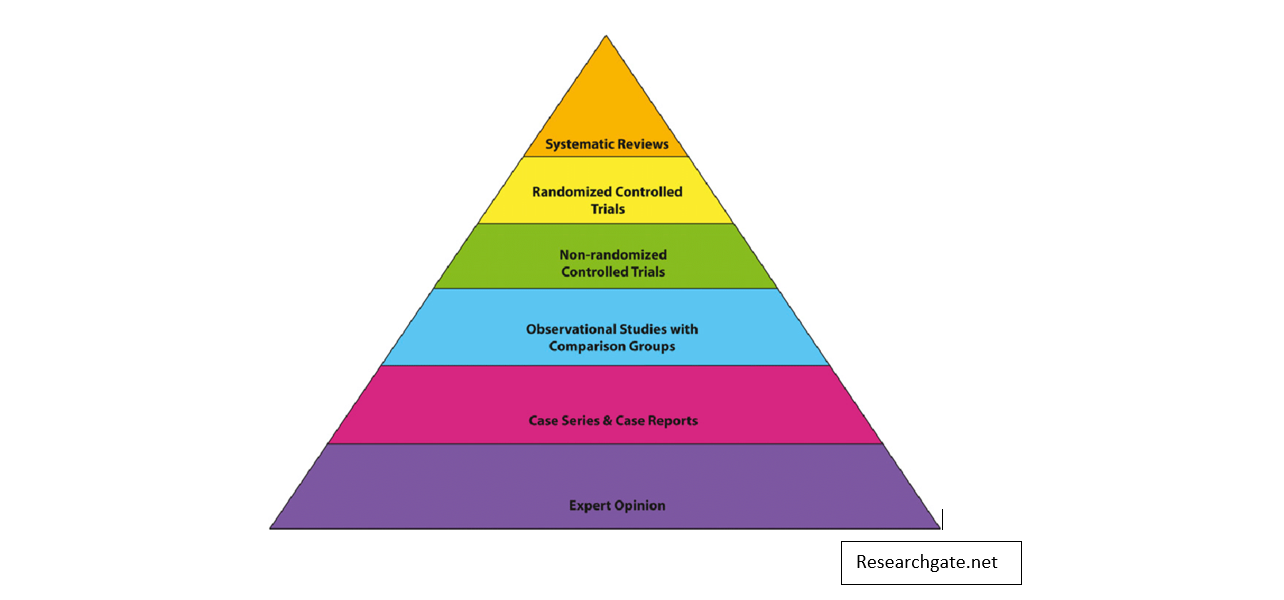
Because you cannot easily randomise people to different groups and therefore conduct a randomised control trial (RCT), we often then rely on “observational studies” to give us the answers. This is a type of study where researchers follow large groups of people and observe changes in certain parameters over time. The issue is often that it can be very hard to control for “confounding factors”. It is difficult to establish which element is responsible for the results, for example, is it red meat consumption that causes extra bowel cancer cases, or is that those people eating meat are also more likely to smoke, or drink more alcohol etc? Real life is much harder to control than a laboratory experiment.
The original intention of EBM was to aim for the highest level of evidence available, not to create an arbitrary yardstick, and dismiss anything that didn’t match up to it.
So while some academics and clinicians are dismissive of the results of observational studies, it is worth pointing out that it is exactly this type of study that taught us the dangers of smoking and the benefits of exercise, both of which I think we can agree have been hugely significant to the health of millions of people.
The key then is to set up your study in such a way that it controls for these confounding factors as much as possible, to use the correct tools to capture the highest quality data, and the proper statistical models to obtain the most reliable results.
Researchers from Australia have now done exactly that. Following on from the previously published work of the Ausimmune Study, which examined the connection between healthy diet and the risk of developing MS, this paper looked at diet quality and the risk of further relapse after someone’s first demyelinating event.
Using well-established models and statistical methodology, the researchers used sophisticated statistical techniques to determine how people’s eating habits clustered into certain patterns. Three dietary pattern groups emerged based on the foods that they were choosing to eat regularly.
When examining the nutritional components of the three dietary groups, the Prudent diet contained higher levels of omega-3, magnesium, potassium, iron and vitamins C and E. It was also associated with lower levels of saturated and total fats (now who would have thought?!).
The investigators then re-assessed the dietary patterns again after 5 years, and reassuringly found that the eating patterns of those 209 people who completed the study had changed very little over time, except for those who started the study either overweight or obese, who were significantly more likely to transition towards the Prudent diet.This means that if any difference in relapse rate was found between the groups, a change in diet was not a factor, thereby strengthening the significance of the role of each individual diet.
When they then compared dietary habits and relapse rates, they found that those eating a more healthy Prudent diet over the study period had a 46% lower relapse rate risk. There was no such reduction in relapse rates for those in either the High-vegetable or Mixed diet groups.
Well, that is true, but this is still an enormously important piece of research. First of all, it is very valuable to have a completely independent data set essentially confirming the findings of Prof. Jelinek’s HOLISM Study, that a diet rich in plant-based foods and fish is protective against MS disease activity. It is extremely reassuring when results are replicated independently, as it makes it much more likely that the observed result was truly significant, and not due to chance, or some unknown factor in one study.
It was also extremely well conducted, not least in the fact that it assessed a person’s diet as a whole, rather than focusing on a specific nutrient This is more representative of the real-world. Despite its relatively small size, the study’s methods were very robust, with consistent and systematic assessments of eating patterns and of relapse and clinical activity, both at the beginning and during follow-up. The fact that over 96% of people completed the study is also very positive for the validity of the results.
Critically, this research was also prospective in nature, so it was designed to follow people BEFORE they developed the outcome in question, in this case, a relapse. This then gives us very real hope that such a dietary intervention can reduce the long-term progression and improve the prognosis of MS.
One criticism of many observational studies is that are retrospective, so examine risk factors for a particular outcome AFTER it has already occurred. This is well known to increase the risk of investigator bias and for confounding factors to play a role in the results, thereby limiting their significance.
To put these results into perspective, many of the currently available disease modifying drugs (DMDs) quote a relapse rate reduction of around 50%, and some significantly less. But eating a healthy diet doesn’t carry the risk of any side effects or the potentially huge monetary costs of drug treatments, and it also protects us from developing many of the other Western diseases that cause so much morbidity and mortality.
Finally, the authors of this particular study read like a “who’s who” of Australian neurologists, now very publicly taking an interest in the role of diet in MS. This is very encouraging to see, and will hopefully lead to many more pwMS hearing the vital message of diet and lifestyle in managing their condition.
To play your part in spreading that message, maybe print a copy of the paper and bring it with you to your next MS appointment, or rather, email it to your MS team in preparation for your next socially distant consultation.
References:
Swank RL and Dugan BB. Effect of low saturated fat diet in early and late cases of multiple sclerosis. Lancet 1990; 336: 37–39.
Black LJ, Rowley C, Sherriff J, et al. A healthy dietary pattern associates with a lower risk of a first clinical diagnosis of central nervous system demyelination. Mult Scler 2018; 25: 1514–1525.
Black LJ, Baker K, Ponsonby AL, et al. A higher Mediterranean diet score, including unprocessed
red meat, is associated with reduced risk of central nervous system demyelination in a case-control study of Australian adults. J Nutr 2019; 149(8): 1385–1392.
Black LJ, Bowe GS, Pereira G, et al. Higher non- processed red meat consumption is associated with a reduced risk of central nervous system demyelination. Front Neurol 2019; 10: 125.
Black LJ, Zhao Y, Peng YC, et al. Higher fish consumption and lower risk of central nervous system demyelination. Eur J Clin Nutr 2020; 74: 818–824
https://www.vox.com/2016/1/14/10760622/nutrition-science-complicated